You’ve tried every “brightening” eye cream, stacked caffeine serums, slept more, slept less, used cold spoons—and those shadows under your eyes are still there. Here’s why: dark circles aren’t one problem. They’re at least four different issues that look similar but need completely different solutions.
Before you throw more money at products, let’s figure out what type you actually have. Because the eye cream that helps your friend might do absolutely nothing for you—and that’s not your fault.
At a Glance
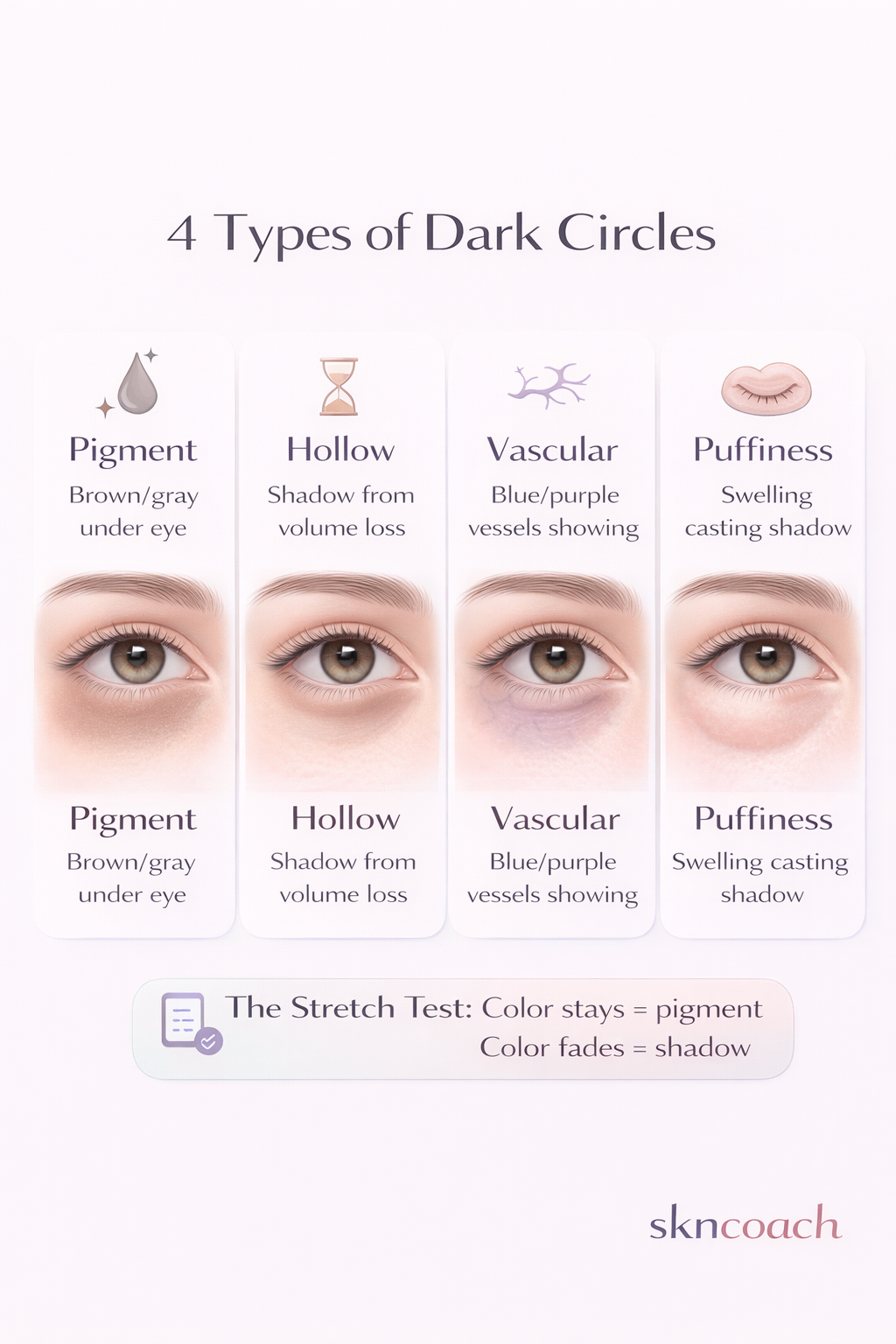
- 4 types: Pigment (brown), Hollow (shadow), Vascular (blue), Puffiness
- First step: Do the stretch test to identify your type
- Pigment/Vascular: Topicals can help (sunscreen, caffeine, vitamin C)
- Hollow: Only fillers add volume—creams can’t
- Mixed types: Most people have more than one factor
The 4 Types of Dark Circles (Quick Self-Test)
Stand in front of a mirror with good lighting (natural daylight is best). Look at the area under your eyes and ask yourself these questions.
Type 1: Pigment-Based (Brown/Gray)
What it looks like:
- Brown, tan, or grayish discoloration
- Color is consistent whether you stretch the skin or not
- Often runs in families
- More common in deeper skin tones
The stretch test: Gently pull the under-eye skin downward. If the color stays the same, it’s likely pigment.
Why it happens:
- Genetics (periorbital hyperpigmentation)
- Sun exposure without protection
- Post-inflammatory hyperpigmentation from eczema or rubbing
- Melasma extending under eyes
Type 2: Hollow/Tear Trough Shadow
What it looks like:
- Deep groove between the lower eyelid and cheek
- Creates a shadow that looks like a dark circle
- More visible when light hits from above
- Gets worse as you age (volume loss)
The stretch test: Gently pull the skin taut. If the “darkness” disappears or significantly fades, it’s a shadow from hollowing—not pigment.
Why it happens:
- Natural aging (fat pad descent, bone resorption)
- Genetics (some people have naturally hollow under-eyes from their 20s)
- Weight loss (facial fat loss)
Type 3: Vascular (Blue/Purple)
What it looks like:
- Bluish, purple, or pink-red tones
- Color becomes more visible when you’re tired or cold
- Often shows blood vessels through thin skin
- Common in very fair skin
The stretch test: When you stretch the skin, you may see fine blood vessels underneath.
Why it happens:
- Thin under-eye skin (genetically or from aging)
- Poor circulation
- Dilated blood vessels
- Allergies causing congestion
Type 4: Puffiness + Shadow Combo
What it looks like:
- Bags or swelling under the eyes
- Shadow cast below the puffy area
- Worse in the morning, may improve as day goes on
- Sometimes accompanied by fluid retention elsewhere
Why it happens:
- Fluid retention (salt, alcohol, crying)
- Allergies (allergic shiners)
- Sinus congestion
- Sleep position (sleeping on stomach/side)
- Aging (fat pad prolapse—fat pushes forward)
Bonus: Allergy/Eczema Darkening
What it looks like:
- Darkening specifically from chronic rubbing
- Often accompanied by slight scaling or dryness
- “Allergic shiners”—dark, puffy appearance with allergies
Why it happens: Chronic rubbing stimulates melanin production. Eczema inflammation leaves PIH (post-inflammatory hyperpigmentation).
What Works by Type (Quick Reference)
Here’s the honest breakdown of what actually helps each type—and what doesn’t.
| Type | What Helps | What Doesn’t |
|---|---|---|
| Pigment | Sunscreen, gentle retinoid, vitamin C/niacinamide, azelaic acid | Most “brightening” creams, quick fixes |
| Hollow | Filler/fat transfer, makeup techniques | Topical products (they can’t add volume) |
| Vascular | Caffeine, cold compress, sometimes lasers, antihistamines | Eye creams alone |
| Puffiness | Caffeine, allergy control, sleep/salt changes, lymphatic drainage | Heavy creams (can worsen) |
| Allergy/rubbing | Stop rubbing, treat underlying allergy, barrier repair | Everything else until you stop rubbing |
Mixed types? Most people have more than one contributing factor. Address each component separately with the type-specific treatments above.
The Boring Routine That Helps Most People
Before chasing expensive specialty products, nail these basics. They address the controllable factors for most types of under-eye concerns.
Morning (AM)
- Gentle cleanser — Don’t tug or rub the eye area
- Moisturizer — Thin layer under eyes is fine, nothing too heavy
- Sunscreen around eyes — This is non-negotiable. UV exposure worsens pigment, thins skin faster, and accelerates aging. Use a mineral sunscreen if the area is sensitive.
- Optional: Caffeine product — If you have puffiness or vascular concerns, apply a thin layer before sunscreen. Give it 60 seconds to absorb.
Evening (PM)
- Gentle makeup removal — Micellar water on a cotton pad, pressed (not rubbed). Or oil cleanser massaged gently.
- Moisturizer — Thicker is fine at night
- Retinoid 2-3x/week — Apply carefully around the orbital bone, not too close to the lash line. If you’re sensitive, skip under-eyes or buffer with moisturizer first.
If Your Under-Eye Area Is Sensitive
Skip the retinoid under eyes entirely until your barrier is healthy. Focus on:
- Fragrance-free moisturizer
- Strict sun protection
- Not rubbing your eyes
Mistakes That Make Dark Circles Worse
You might be sabotaging yourself without realizing it.
Rubbing and Tugging
Every time you rub your eyes, you’re:
- Stimulating melanin production (more pigment)
- Causing micro-trauma that leads to inflammation
- Breaking down collagen in already-thin skin
Fix: If you have allergies, treat them. If you rub unconsciously, become aware. Remove makeup by pressing, not wiping.
Harsh Makeup Removal
Waterproof mascara removed with aggressive rubbing = the perfect storm for under-eye darkening.
Fix: Use an oil-based remover or micellar water. Let it sit on closed eyes for 30 seconds before gently wiping. Use soft pads, not rough cotton.
Retinoid Too Close + Too Strong
Tretinoin or retinol applied right up to the lash line = irritation, peeling, and paradoxically more darkness from inflammation.
Fix: Apply retinoid to the orbital bone only (the bony ridge around the eye socket). Product will migrate naturally. Start with low strength. Skip if irritated.
Over-Exfoliating
Chemical exfoliation around the eyes (glycolic, salicylic) thins the already-thin skin, increases sensitivity, and can cause PIH in darker skin tones.
Fix: Keep acids away from the immediate under-eye area. The rest of your face can handle them—this area often can’t.
Dehydration + Heavy Concealer
Dehydrated under-eye skin + thick concealer + setting powder = creasing and cakiness that draws attention to the very thing you’re trying to hide.
Fix: Hydrate first (thin moisturizer or hydrating serum). Use the minimum concealer needed. Skip powder or use the tiniest amount pressed on.
Ignoring allergies: Chronic allergies = chronic rubbing + chronic inflammation = chronic dark circles. Treating the underlying allergy with antihistamines or nasal corticosteroids is more important than any eye cream.
When to See a Professional
Eye creams and routines can only do so much. Here’s when it’s time for expert help.
Immediate Medical Attention
Seek help right away if you have:
- Sudden one-sided swelling — Could indicate infection or other serious issue
- Pain around the eye — Not normal with dark circles
- Vision changes — Any blurriness, floaters, or vision loss
- Fever with eye symptoms — Possible orbital infection
These are not cosmetic concerns—they’re potential medical emergencies.
Dermatologist Consultation
See a derm if:
- You’ve tried OTC options for 8-12 weeks with no improvement
- You have persistent eczema or irritation around eyes
- You want to discuss prescription options (stronger retinoids, bleaching agents)
- You have skin of color and want guidance on pigment-safe treatments
Cosmetic Filler Consultation (For Hollow Under-Eyes)
If the stretch test confirmed your dark circles are from hollowing, topical products won’t help. Consider filler if:
- You want structural improvement, not just concealment
- You understand it’s temporary (6-18 months typically)
- You choose a skilled injector (this matters enormously—see below)
Why injector skill matters:
The under-eye area is technically challenging:
- Thin skin shows every imperfection
- Blood vessels and delicate structures nearby
- Risk of Tyndall effect (bluish color from filler placed too superficially)
- Risk of lumps, asymmetry, and vascular occlusion
Who to look for:
- Oculoplastic surgeons (specialize in the eye area)
- Experienced dermatologists or plastic surgeons who do high volumes of tear trough work
- Ask to see before/after photos specifically for tear trough filler
Start conservative: Less is more. You can always add—you can’t easily remove. A good injector will under-correct on the first visit.
Read more: Tear Trough Filler vs Eye Cream: What Each Can Fix
FAQ
Do eye creams actually work?
It depends on what you mean by “work.”
Eye creams can:
- Hydrate the area
- Deliver active ingredients (retinoid, vitamin C, caffeine, niacinamide)
- Temporarily plump fine lines
- Reduce puffiness slightly
Eye creams cannot:
- Fill in hollow tear troughs
- Permanently eliminate genetic pigmentation
- Replace lost volume
Bottom line: Eye creams are just face creams in smaller jars. If a product has the right active ingredients and you tolerate it well around your eyes, it can help—but don’t expect miracles for structural issues.
Can tretinoin go under the eyes?
With caution.
Tretinoin can help with:
- Fine lines and crepey texture
- Mild pigmentation
- Overall skin quality
But the under-eye area is thin and sensitive. Guidelines:
- Start with the lowest strength (0.025%)
- Apply to the orbital bone only, not up to the lash line
- Use 1-2x per week initially
- Buffer with moisturizer if irritation occurs
- Skip entirely if you have eczema or chronic sensitivity
Some people can’t tolerate retinoids under the eyes at all—and that’s okay. Focus on sun protection and gentle hydration instead.
Is it “loose skin” or dark circles?
These are different issues:
- Loose skin/crepiness: Fine lines, wrinkled texture, thin skin that looks papery. Caused by age, sun damage, and collagen loss.
- Dark circles: Discoloration from pigment, hollowing, vessels, or puffiness.
You can have both. Loose skin benefits from:
- Retinoids
- Sun protection
- Peptides
- Eventually, tightening procedures (laser, RF microneedling, or surgery)
Dark circles need their type-specific treatment (see above).
Why are my dark circles worse some days?
Common fluctuating factors:
- Sleep: Both too little AND too much can cause puffiness
- Salt intake: Causes water retention
- Alcohol: Dehydrates and dilates blood vessels
- Allergies: Flare-ups = rubbing + congestion
- Crying: Salt + rubbing + inflammation = temporary darkness
- Sleeping position: Sleeping face-down or on one side pools fluid
- Hormonal changes: Some people notice darker under-eyes around menstruation
The color might not actually change—but puffiness and swelling affect how shadows fall.
Can makeup help while I work on this?
Absolutely. A few tips:
- Color correct first: Peach/orange tones cancel blue-purple. Pink cancels gray. Salmon works for brown-gray on medium tones.
- Use minimal product: Thin layers prevent creasing. Less is more.
- Don’t set with heavy powder: A light dusting only, or skip entirely.
- Hydrate first: Thin moisturizer under everything.
- Avoid shimmer: Can emphasize texture and crepiness.
The Bottom Line
Dark circles are frustrating because there’s no one-size-fits-all solution. But now you know why: they’re not one problem.
Your action plan:
- Identify your type (or types) using the stretch test and mirror check
- Nail the basics: Gentle care, no rubbing, religiously use sunscreen
- Add targeted treatment: Based on your specific type
- Set realistic expectations: Improvement, not perfection
- Know when to seek help: Some issues need procedures, not products
Looking to build a minimal routine that adapts to your skin’s needs—including eye-area concerns? skncoach creates personalized plans based on your specific skin type and goals.
Related reads:
- Tear Trough Filler vs Eye Cream: What Each Can and Can’t Fix
- Caffeine for Under-Eyes: Does It Work or Is It Hype?
- Rosacea Routine That Actually Calms Redness
This content is for informational purposes only and does not replace professional medical advice. If you have concerns about your skin or eyes, please consult a dermatologist or ophthalmologist.

